Progressive reduction in growth hormone (hGH) production and secretion beginning shortly after young adulthood is an early endocrine characteristic of aging in humans and animals. Over time lowering levels of this hormone contributes to many of the undesirable aspects of senescence. These include changes in body composition favoring fat over muscle, bone loss, and increased risk for intrinsic diseases such as stroke, circulatory disorders, diabetes and others.
But why are hGH and other important hormones and essential metabolites reduced during aging? And once knowing the reason, what is the best way to treat this endocrine deficiency? The answer lies in understanding the nature of how our bodies transform throughout life and how those changes negatively affect neuroendocrine function.
Change or remodelling of the body is a characteristic of every sexually reproducing animal because survival requires that it transform from a single fertilized egg into a complex multicellular organism capable of independent function. Because of this requirement for dynamic and integrated transformation, a developmental program capable of coordinating change evolved in the earliest multicellular organism. The genetically based developmental program was selected and conserved throughout the evolution of complex animal species because it guaranteed individual survival until reproduction and assurance of subsequent generations thereafter. However, one of the most basic characteristics of evolution is that after reproductive capability is reached, natural selection becomes inoperable (1, 2). This means that inclusion of new genes into existing programs becomes highly unlikely after young adulthood, the final stage of development following acquisition of reproductive competence. The significance of this fact is that expression of genes orchestrating dynamic transformation of the body to final maturation continues beyond the time when the organism is capable of reproducing. Thus, a “stop signal” to terminate “developmental inertia” or the tendency to change after development is complete could not evolve (3). Furthermore, because the genes carrying information to guide and coordinate the dynamic transformation of development are depleted of that information at maturity, further remodelling of the body is unguided. This means that change occurring after maturation is no longer adaptive as it was during development, because adult animals unlike those that are developing require internal stability or homeostasis not change, in order to sustain optimal health and vitality. Thus, unremitting and undirected somatic or bodily change resulting from residual expression of specific developmental genes continues throughout adulthood.
As it does, essential interactions between various components of the body that function sequentially, i.e. step 1 to precede step 2, to precede step 3, etc. become disordered. As a result, distinct rhythms that are essential for health and vitality slowly erode, progressively increasing internal disorder and physiological chaos that is characteristic of aging. It is this post-maturational decay of time structure resulting from residual developmental change that slowly erodes function within essential elements of the body (4). The neuroendocrine system which consists of the brain, pituitary gland and much of the body, ranging from endocrine glands, e.g., thyroid, adrenals, gonads, etc. as well as muscle, bone, skin, heart, kidneys, etc. is especially impacted by post-maturation developmental inertia because signals coming from higher levels must reach their target cells at times when the cells are most ready to be stimulated. As internal time structure decays and signaling becomes uncoupled, then responses become less and less robust. This is why hGH production declines during aging bringing with it the detrimental effects we associate with growing older.
Age-related hGH insufficiency and its detrimental consequences have been recognized for over two decades. In 1990, Rudman and colleagues showed that many of these undesirable effects on the body could be opposed by administration of recombinant hGH (5 ). Because of its efficacy, such replacement therapy dominated approaches to age-management disorders well into the 21st century. However, as the result of abuse and overdosing it eventually became apparent that this pharmacological approach to growth hormone replacement therapy had its drawbacks. First of all, recombinant hGH is administered by injection at a fairly standard dose that became adopted without sufficient scientific basis. This “one size fits all” approach invariably would be too much for some individuals while not enough for others.
Furthermore, and perhaps more importantly, recombinant hGH is injected as a bolus that rapidly elevates and sustains serum levels in a way that is “unnatural” to the body. As seen in Figure 1 (6), whether the hormone is injected under the skin or into a vein, elevated blood levels are sustained for several hours (iv) up to a day (sc).
Figure 1:
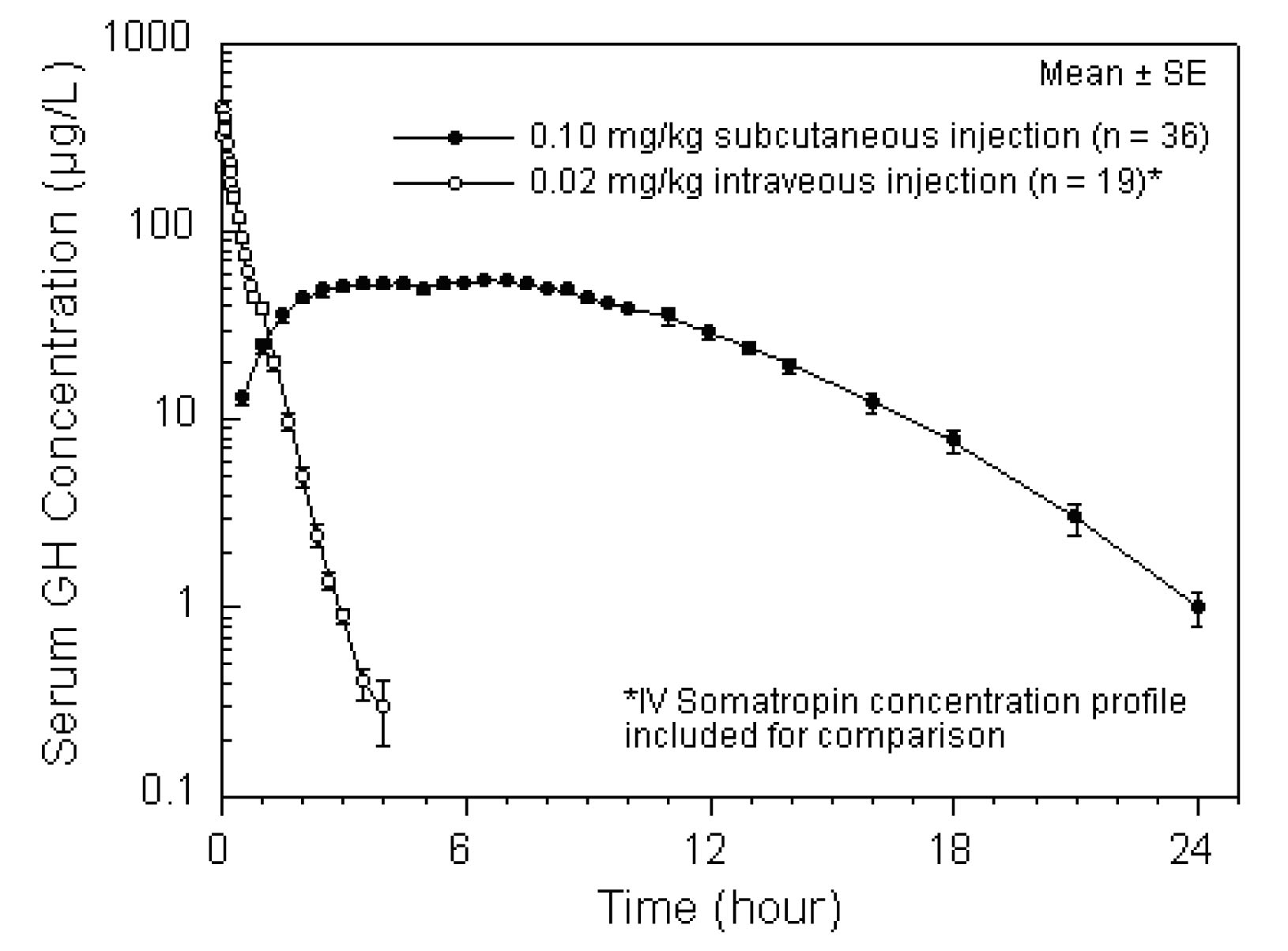
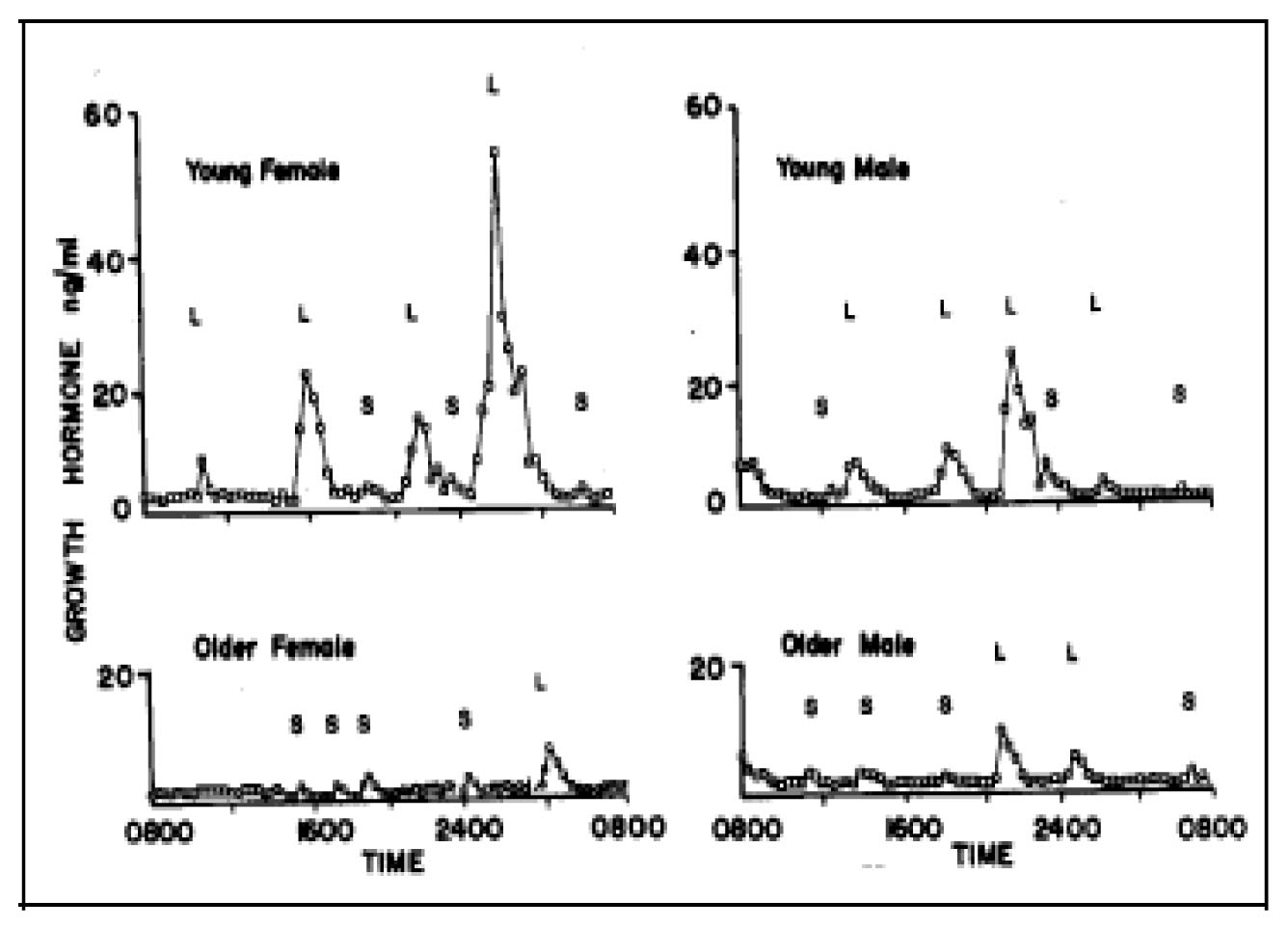
There are several problems with this pharmacological approach considering that “natural” secretion of hGH from the pituitary gland is episodic, i.e. in intermittent bursts throughout the day. The naturally occurring patterns for young and older individuals are shown in Figure 2 (7). Note that with advancing age, the timed and spontaneous secretions of hGH from the pituitary gland are blunted and reduced in frequency.
Figure 2:
Thus, the pharmacological approach to growth hormone therapy in anti-aging medicine increases the risk for overdose as well as for tachyphylaxis, the tendency for receptors to become desensitized by overstimulation.
Another important disadvantage of the pharmacological approach is that it may accelerate age-related deterioration of brain and pituitary function through the process of negative feedback or end product inhibition. First of all we should recognize that the growth hormone neuroendocrine axis is a complex hierarchy consisting of several essential elements including brain cells that secrete growth hormone releasing hormone, pituitary cells that produce and secrete hGH, the liver which produces IGF-1, the effects of which represent the action of hGH and many other ancillary sites throughout the body. (Figure 3).
Figure 3:
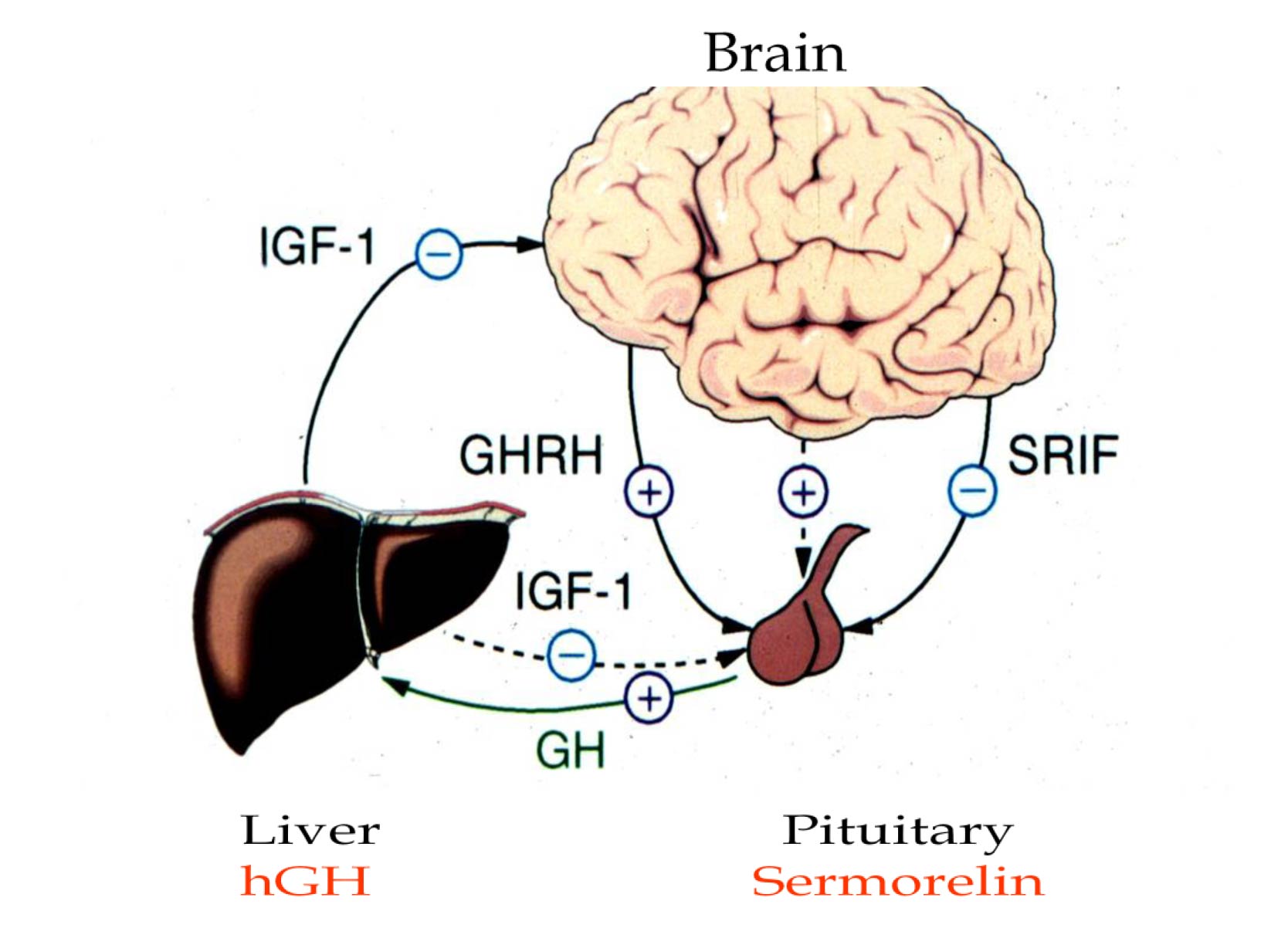
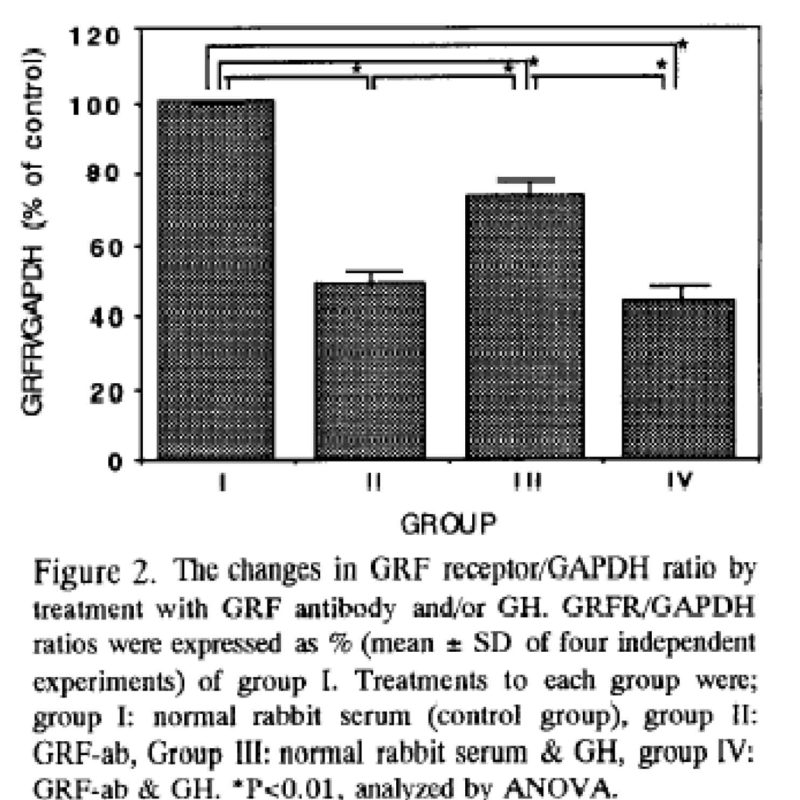
These elements of the hGH neuroendocrine system require proper stimulation to remain healthy, viable and functional entities. It is obvious from brief examination of Figure 3 that when hGH is administered pharmacologically, it goes straight to the liver, bypassing the higher centers. This lack of action by the brain and pituitary gland as well as negative feedback influence of IGF-1, a hormone produced by the liver under the influence of hGH causes the higher centers to further cease function. Thus, when hGH is administered pharmacologically, some of its direct effects on the body are realized, while others in the brain and pituitary gland are shut down. This “disuse atrophy” is analogous to never using the muscles of your body, but rather simply sitting all your life and having things brought to you. Eventually, your muscles will atrophy and become incapable of reactivation. In consideration of this fact, a very important aspect of holistic, anti-aging therapy involving hormones is to try whenever possible to include the highest level of function in treatment. Disuse atrophy of the pituitary gland can be seen when receptors for growth hormone releasing hormone or its analog, sermorelin, decline when recombinant hGH is administered pharmacologically (Figure 4 [8]). As seen in group 3, GHRH receptors are reduced when compared to controls represented in group 1.
Figure 4:
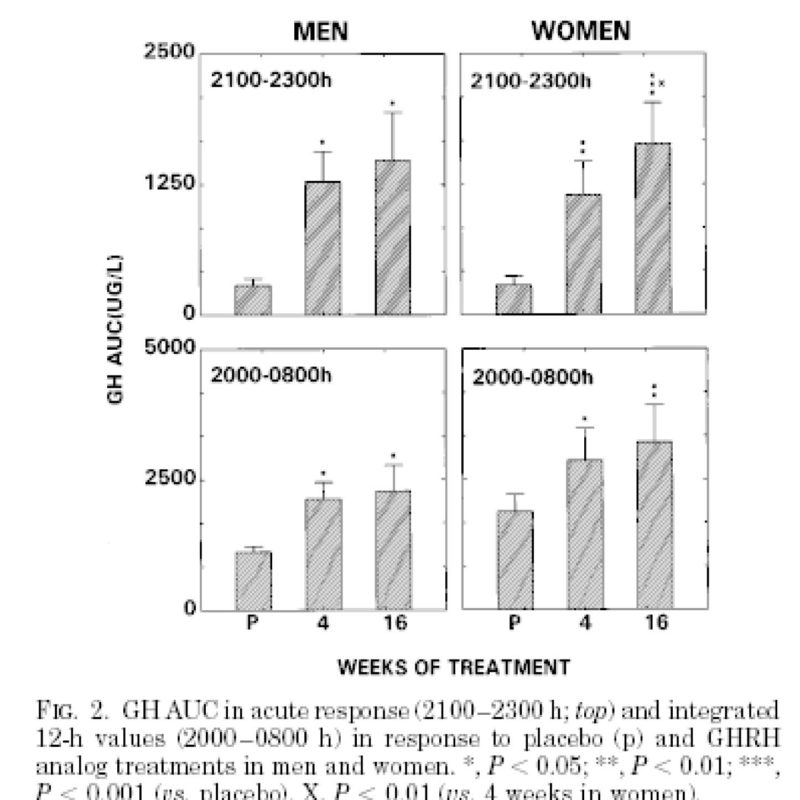
In contrast, administration of sermorelin rather than recombinant hGH is a more beneficial, holistic and physiological approach to growth hormone therapy in anti-aging medicine. The reasons for this conclusion is that sermorelin incorporates more of the hGH neuroendocrine axis than recombinant hGH and has been shown to be effective in making the body produce its own hGH rather than replacing it with the recombinant product. As seen in Figure 5 (9), hGH concentrations increase after weeks of sermorelin administration. This increase demonstrates that treatment restored GHRH receptors and rejuvenated the pituitary cells capable of producing and secreting hGH.
Figure 5:
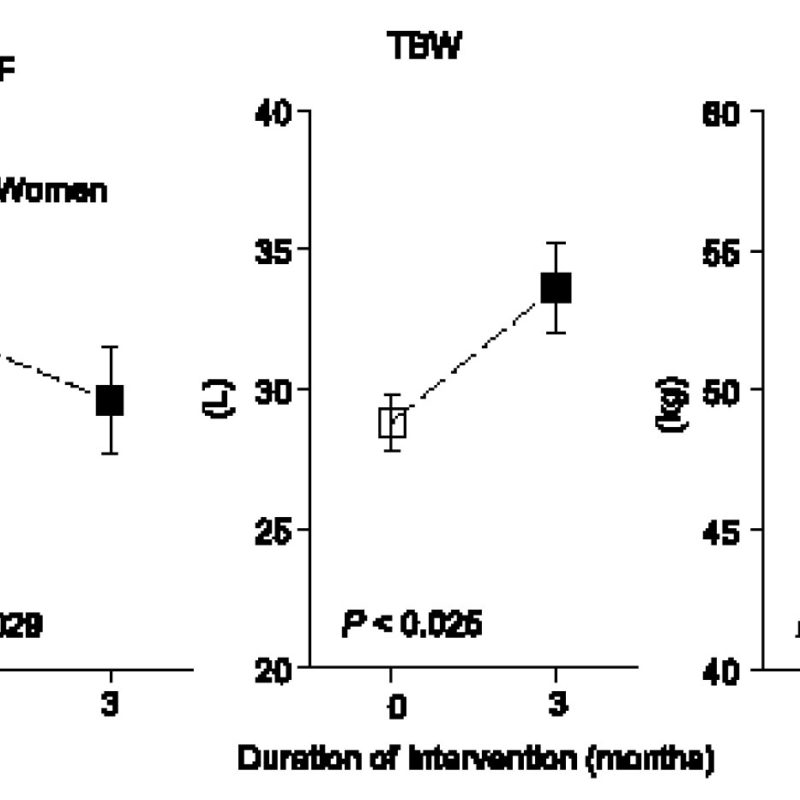
As a result increased concentrations of hGH resulting from sermorelin administration improves body composition as shown in Figure 6 (7). After three months of treatment, abdominal visceral fat (AVF) decreased, while total body water (TBW) and lean body mass or muscle (LBM) increased in elderly subjects.
Figure 6:
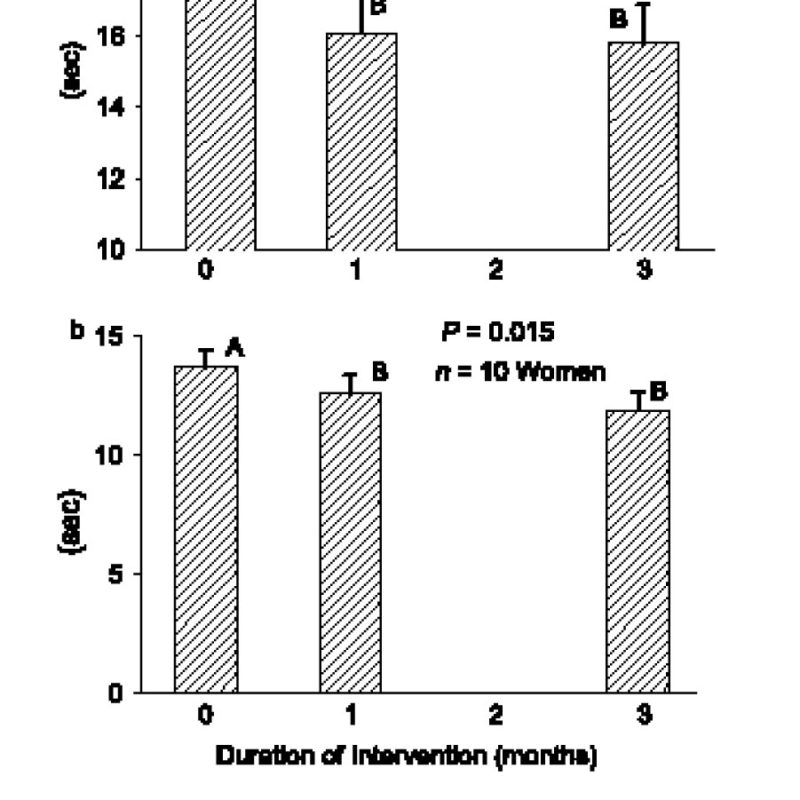
Furthermore, as a concomitant of these positive changes in body composition, physical performance improved significantly. As seen in Figure 7 (7), the ability of post-menopausal women to perform timed physical tasks improved as indicated by the fact that they could climb stairs faster and to walk distances more rapidly than before treatment.
Figure 7:
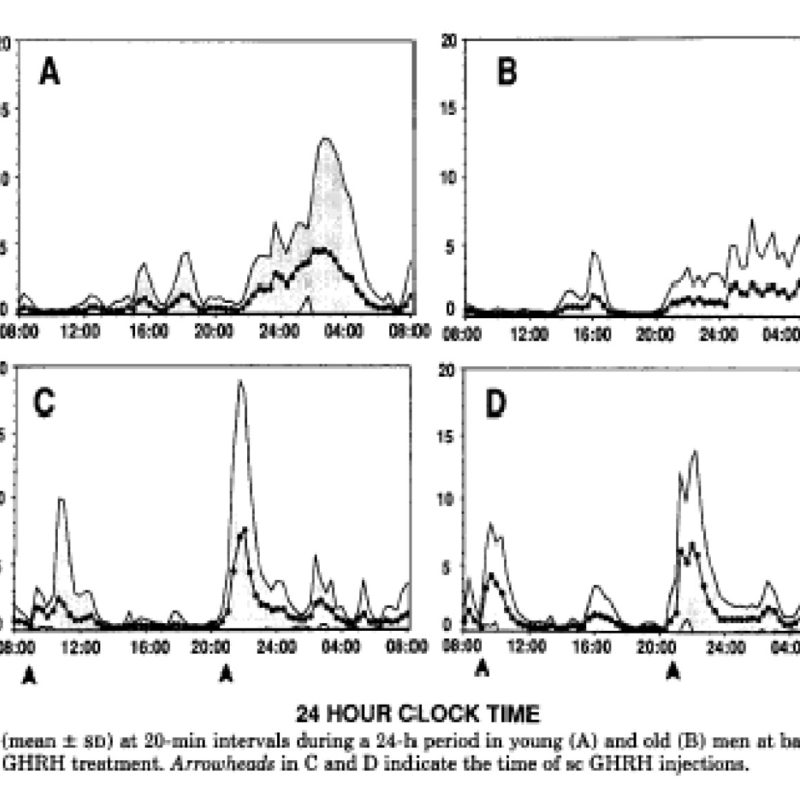
Sermorelin administration also restores normal episodic release of growth hormone and thereby demonstrates its ability to support more youthful feedback relationships. The effect of sermorelin on these episodic hGH release patterns is demonstrated in Figure 8 (10). The graphs in panel A and B show the normal patterns of daily, episodic hGH secretion in young and old men, respectively. Administration of low and high dosage sermorelin to old men as shown in panels C and D, respectively restored previously blunted to more youthful, higher amplitude patterns of spontaneous secretion.
Figure 8:
Thus in summary, unlike exogenous rhGH that is foreign to the body, sermorelin simulates the patient’s own pituitary gland by binding to specific receptors to increase production and secretion of endogenous hGH. Because sermorelin increases endogenous hGH by stimulating the pituitary gland it has certain physiological and clinical advantages over hGH that include:
Its effects are regulated by negative feedback involving the inhibitory neurohormone, somatostatin so that unlike administration of exogenous, rhGH, overdoses of endogenous hGH are difficult if not impossible to achieve,
Because of the interactive effects of sermorelin and somatostain, release of hGH by the pituitary is episodic or intermittent rather than constant as with injected rhGH. Because sermorelin induced release of pituitary hGH is not “square wave” but instead simulates more normal physiology, tachyphylaxis is avoided.
Sermorelin stimulates pituitary gene transcription of hGH messenger RNA, increasing pituitary reserve and thereby preserving more of the growth hormone neuroendocrine axis, which is the first to fail during aging (11).
Daily administration before bedtime may provide a zeitgeber to reinforce the original ordered stimulus of the brain/pituitary axis to release hGH during sleep, thus helping to restore temporal order, the cause of age-associated hGH insufficiency.
Pituitary recrudescence resulting from sermorelin helps slow the cascade of hypophyseal hormone failures that occurs during aging thereby preserving not only youthful anatomy but also youthful physiology (12).
Traditionally, peptides are administered by injection so as to avoid degradation in the gastrointestinal tract thereby increasing bioavailability. Also, because of shortages of material that originally occurred in product development, peptides such as sermorelin were administered in very small intravenous doses.
Of course, iv injections are difficult to perform on one’s self and could be dangerous for those not familiar with the technique. However, as product availability increased, subcutaneous dose ranging tests were performed. The data showed that bioavailability by this route was greater than previously expected making it a practical method for treating age-associated growth hormone insufficiency.
As a result, sermorelin started gaining favor as a physiological approach to hGH replacement therapy in 2007. Since then its safety and efficacy have been the basis for an ever expanding use of the product by age management, health care practitioners. Over the course of the past four + years, thousands of people have received sermorelin therapy for hGH insufficiency, enjoying the benefits of holistic growth hormone replacement without suffering the potential side effects associated the recombinant product.
Perhaps the only drawback to date has been its route of administration. Undoubtedly, there are many people who are averse to the requirement for daily injections of sermorelin, even if they are of small volume and administered with extremely fine needles. As a result, many individuals who could benefit from sermorelin as part of their anti-aging regimen unfortunately do not take advantage of its benefits. Until just recently, the idea that sermorelin might be bioavailable by non-parenteral routes was just as foreign as when previously it was doubted to be effective by subcutaneous administration. However, recognizing that the peptide is relatively small and with the advent of modern pharmaceutical methods for enhancing absorption, a sublingual or “under the tongue” formulation of sermorelin was created.
The logic behind that effort was that chemicals placed in contact with the mucous membrane beneath the tongue can diffuse through it and enter the venous circulation directly. In contrast, peptides swallowed into the stomach and intestines risk digestion by degrading enzymes and are also subject to “first pass metabolism” in the liver before entering the general circulation. Thus, even if sermorelin were capable of being absorbed from the gut without losing all of its activity to enzymatic cleavage, metabolism in the liver would almost surely prevent passage of any active component into the bloodstream. As a result, various formulations of sermorelin in vehicles capable of improving its passage into the circulation from under the tongue were investigated since this route would most closely resemble subcutaneous delivery without injection.
Recently, a unique combination of active ingredients and excipients has been created that provides sufficient bioavailability of sermorelin to achieve desired clinical and laboratory effects. Thus, individuals who previously avoided using this growth hormone secretagogue as a regular part of their anti-aging program because of the need to inject can now enjoy its benefits without enduring the pain and psychological stress of needle administration.

